










Use of Bladder ultrasound
- 2023-02-19
- 1622
- Sonostar Technologies Co., Limited
"Do I really need to catheterize my patient to check residual urine?" The answer to this question in many facilities is still "yes." However, a relatively new piece of equipment may eliminate catheterization for checking residual urine. A facility may not have purchased a bladder scanner because the cost may be prohibitive (approximately $8,000 each), or it may be that the value of using a bladder scanner has not been recognized. Indwelling urinary catheters will continue to be utilized, but the bladder scanner can be used to eliminate in-and-out catheterization to check a patient's residual urine volume or to assess the need to catheterize the patient who has not voided for a period of time, as when assessing postoperative urinary retention. The bladder scanner creates an ultrasound image of the patient's bladder, and calculates and displays the urine volume (Patraca, 2005).
Checking post-void residual (amount of urine left in the bladder within 10-15 minutes after voiding) is important in assessing patients who are suspected of incomplete bladder emptying or urinary retention. An elevated post-void residual may lead to an increased risk of acute urinary retention, urinary tract infection, pyelonephritis, hydronephrosis, or renal insufficiency (Newman, 2003).
Prior to the development of the ultrasound bladder scanner, the only way to determine if the bladder was completely empty was either to palpate and percuss the suprapubic area or perform intermittent catheterization. With percussion, a dull sound may represent fluid. Dullness of the bladder to the level of the umbilicus indicates at least 500 ml of urine. Palpation may reveal a mid-line mass extending upward from the suprapubic area in bladders with more than 500 ml (Newman, 2003). This is the most inaccurate method of determining bladder volume.
Intermittent catheterization is accurate but it has several disadvantages. First and foremost, because it is an invasive procedure with the potential for introducing bacteria into the urethra and bladder, catheterization potentially could cause a urinary tract infection (Ribby, 2006). Catheterization also can be uncomfortable and embarrassing for the patient, time consuming for the nurse, and costly for the institution (Stevens, 2005).
The BladderScan[TM] is a portable, noninvasive ultrasound instrument that measures bladder volume. It provides a precise reading of a patient's bladder volume, thereby preventing unnecessary catheterization. The positive outcome for using an ultrasound bladder scanner is the reduction of nosocomial urinary tract infection and decreased nursing time. It is a cost-effective strategy that eliminates potential trauma to patients.
Clinical Indications
* Assess post-void residual, urinary retention, or incomplete bladder emptying
* Prevent urinary retention following indwelling catheter removal
* Assist with bladder retraining by determining need to void based on bladder volume
* Determine bladder volume in patients who have incomplete bladder emptying or who are on scheduled catheterization times to drain the bladder
* Monitor postoperative patient or in the patient who is physically unable to void (for example, after spinal cord injury)
* Determine bladder volume in a patient with decreased urine output
* Assist in implementing toileting program by determining amount of urine in the bladder when attempting to toilet a patient
Potential Inaccurate Readings
Factors that may cause inaccurate readings include morbid obesity; use of an inadequate amount of ultrasound gel; improper aiming of the scan head (the bladder is partially or wholly outside the field of vision); moving the probe during the scan; and the presence of scar tissue, incisions, sutures, and staples (Newman, 2003).
Use of the Ultrasound Bladder Scanner
Because several models of bladder scanners are available, it is best to reference the manufacturer's guidelines for use. The following are general directions based on a common type of scanner.
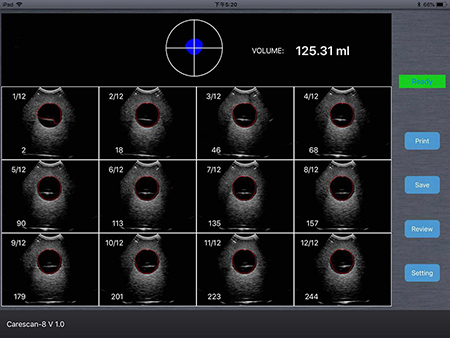
After the nurse turns on the machine and presses the "scan" button, some type of graph will be visible to give a picture description of the quantity of urine in the bladder. The nurse will need to indicate the patient's gender, using "female" only if the patient has not had a hysterectomy and selecting "male" for men or for women who have had a hysterectomy. With this done, the machine does not have to discriminate between the bladder and the uterus as two hollow organs. The scan head should be wiped with a hospital-approved disinfectant. After gently palpating the patient's symphysis pubis, the nurse will apply ultrasound gel midline on the patient's abdomen (about 1-1.5 inches above the symphysis pubis) and place the scan head on the gel. Alternately, gel can be applied directly to the scan head and then positioned on the patient's abdomen over his or her bladder. Aiming the scan head toward the patient's bladder, the nurse should watch the image on the scanner screen. The "scan" button should be pressed and held until a beep is heard. The volume measurement will appear on the screen. If the initial image is not centered, the scan head should be repositioned and the procedure repeated until the bladder is in the center of the graph; repeating this noninvasive procedure does not harm the patient. Most machines allow a printout of results if needed.
Documentation should include the reasons for using the bladder scanner (for example, patient unable to void postop; checking post-void residual), the urine volume indicated, the patient's response to the procedure, any physician notification, and if ordered, any follow-up treatment.
References
Newman, D. (2003). Using the BladderScan[R] for bladder volume assessment. Retrieved May 30, 2006, fromhttp://www.seekwellness.com/ incontinence/using_the_bladder scan.htm
Patraca, K. (2005). Measure bladder volume without catheterization. Nursing 2005, 35(4), 46-47.
Ribby, K. (2006). Decreasing urinary tract infections through staff development, outcomes and nursing process. Journal Nursing Care Quality, 21(2), 194-198.
Stevens, E. (2005). Bladder ultrasound: Avoiding unnecessary catheterizations. MEDSURG Nursing, 14(4), 249253.
Vanessa Altschuler, BSN, RN, is a Staff Nurse, Orthopedic-Neuro-Trauma North Broward Medical Center Deerfield Beach, FL.
Lisa Diaz, BSN, RN, is a Staff Nurse, Orthopedic-Neuro-Trauma, North Broward Medical Center, Deerfield Beach, FL.












 网站首页
网站首页 产品中心
产品中心 服务支持
服务支持 联系咨询
联系咨询